Hand Arthritis
Arthritis in the hand is very common, particularly in patients over 50 years of age. Arthritis – in any joint in the body – is degeneration of the cartilage. “Arth” (joint) “itis” (inflammation) can have numerous causes, including trauma to a joint, infection, and most commonly, age-related wear and tear of the joint cartilage (“degenerative arthritis”). This is in contrast to Rheumatoid Arthritis which is an auto-immune condition in which the body’s own immune system attacks joint cartilage, causing degeneration of the cartilage. Arthritis caused by Rheumatoid Arthritis has become less common in the last decade with the advent of medications which can prevent the body from attacking its own joints.
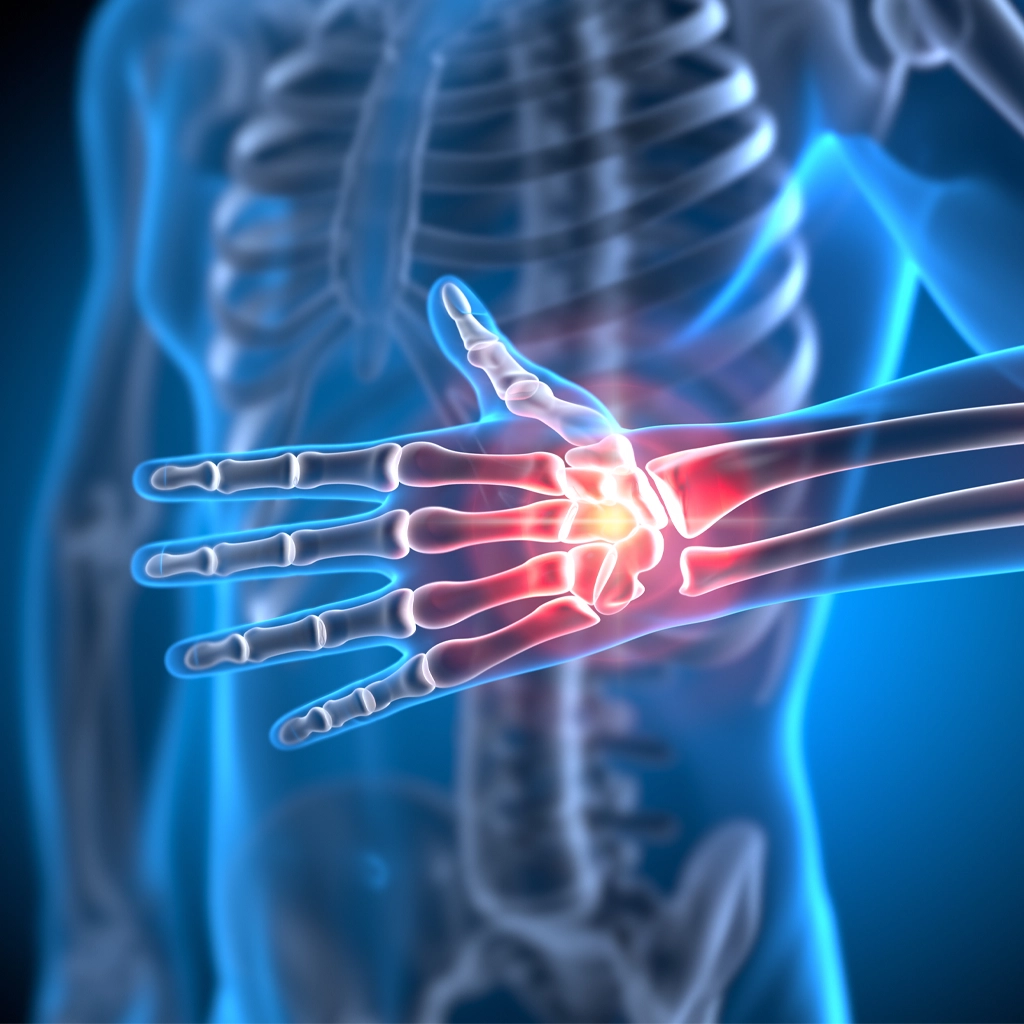
Arthritis of the hand can affect any joint of the hand or wrist. The joint that most commonly becomes arthritic in the hand is the joint at the base of the thumb (the carpometacarpal joint or “CMC” joint). Arthritis causes pain, stiffness and with advanced degeneration, deformity of the joint.
The first line of treatment for arthritis (of any joint) is activity modification. Avoid activities that aggravate the pain in the joint. Non-steroidal anti-inflammatory medications are very commonly used to treat pain associated with arthritis. Unfortunately, there is no way to reverse the changes that occur to the joint when it becomes arthritic. Cartilage is very durable but once it deteriorates, there remains no method by which the cartilage can be restored to new.
A cortisone injection can provide temporary (weeks to months) of relief from the pain associated with arthritis. A patient can receive a cortisone injection two or three times per year. If given too often, cortisone can cause permanent damage to the tendons and ligaments surrounding the joint. This is why doctors are judicious in how often they administer cortisone.
For thumb CMC joint arthritis, a splint can help alleviate the symptoms. If a patient fails to improve with splinting and an occasional cortisone injection, surgery can provide long-term relief. There are several surgical techniques for thumb CMC arthritis. A common technique is removal of the trapezium bone (the carpal bone that articulates with the base of the thumb metacarpal at the CMC joint). A soft tissue spacer is sometimes place in the void left by the removed bone, to prevent subsidence (settling) of the thumb. Generally, the thumb is immobilized for 4-6 weeks after surgery. Thereafter, the patient is placed in a removable splint, arranged for hand therapy and encouraged to get the thumb moving. Full recovery from the procedure is, on average, 6 months.
For other joints in the hand, splinting is generally not particularly helpful for arthritis. Cortisone injections can be helpful but there is often not a lot of space in the joint into which the doctor can place cortisone. If a patient fails conservative management for arthritis in the hand, the surgical options include fusing the arthritic joint or replacing the joint with a rubber (or metal) joint. The advantage of a fusion is that it is a one and done surgery; after fusing the joint (removing the remaining cartilage and compressing the bones together, to heal, like a fracture), the pain should be gone forever. The drawback is that the patient will lose motion at that joint.
The advantage of a joint replacement is that it can preserve motion of the joint. The disadvantage is that it is like a tire. It will wear out with time and will either require a revision joint replacement or a conversion to a fusion. Thus, if a patient opts for a finger joint replacement, then the patient should be made aware of the fact that a second surgery may be necessary in the future, to either replace the joint replacement or to fuse the joint.
Joint surgeries for hand arthritis are performed under general anesthesia. Surgical time is, on average, about an hour per joint. Full recovery is 3-6 months.